ILLINOIS
ENVIRONMENT
)
PROTECTION
AGENCY
)
)
Complainant,
)
)
v.
)
AC
09-39
)
(IEPA
No.
18-09-AC)
DONALD
SAPP,
)
(Administrative
Citation)
)
Respondent,
ADMINISTRATIVE
HEARING
AUGUST
11,
2009
10:30
am
HEARING
DOCUMENTS
Attached
are
physical
documents
that
I,
Donald
Sapp,
would
respectively
ask
to
be
entered
in the
record
for
the
August
11,
2009
telephone
Administrative
Hearing.
I
would
further
request
that
these
materials
be
made
a
part
of
my
IEPA
No.
1
8-09-AC
file.
Please
initiate
the
Hearing
conference
call
at
217-285-1987
(land
line)
rather
than
217-437-5861
(cell).
My
cell
phone
does
not
always
have
the
best
reception
so
the
land
line
would
be best.
01742
5-308-286
h
01
31
MAYO
CLINIC
Monthly
StmenI
I
cij
Accoun;
Page
2
Statement Date:
12/27/2007
Patient
Name
Mayo
Clinic Number/Visit Number
Dates
of Service
Insurance
Place
of Service
Account
Claims
Personal
Transaction
Detail/Description
Activity
Pending
Responsibility
SAPP,
DONALD
RAY
5-308-286
Visit
7115
04/25/2007
- 04/30/2007
Mayo
Clinic Rochester
Previous Balance
$
2,625.45
Visit
Balance
$
2,625.45
Insurance
Pending
$
0.00
Amount
Due
$
2,625.4
SAPP,
DONALD RAY
5-308-286
Visit 7121
05/01/2007
- 05/01/2007
Mayo
Clinic
Rochester
Previous
Balance
$
26.81
Visit
Balance
$
26.81
Insurance
Pending
$
0.00
Amount
Due
$
26.8:
SAPP,
DONALD
RAY
5-308-286
Visit
7129
05/10/2007
- 05/10/2007
Rochester
Methodist
Hospital
Previous
Balance
$
23.90
Visit Balance
$
23.90
Insurance
Pending
$
0.00
Amount
Due
$
23.9i
SAPP,
DONALD
RAY
5-308-286
Visit
7130
05/10/2007
- 05/10/2007
Rochester
Methodist Hospital
Previous
Balance
$
421.66
Visit
Balance
$
421.66
Insurance
Pending
$
0.00
Amount
Due
$
421.6
J1/42
5-3Ub-236
h
Ui
\JJ
J)
IVIAYO CLINIC
MonthEv
J
Siatement
of Acconi
Page
3
Statement
Date:
12127/2007
Patient Name
Mayo
Clinic
Number/Visit
Number
Dates
of Service
Insurance
Place of
Service
Account
Claims
Personal
Transaction
Detail/Description
Activity
Pending
Responsibility
SAPP,
DONALD RAY
5-308-286
Visit
7131
05/10/2007
05/10/2007
Mayo Clinic
Rochester
Previous
Balance
$
184.91
Visit Balance
$
184.91
Insurance
Pending
$
0.00
Amount Due
$
184.9]
SAPP, DONALD
RAY
5-308-286
Visit
7140
05/10/2007
- 05/11/2007
Mayo Clinic
Rochester
Previous
Balance
$
89.05
Visit Balance
$
89.05
Insurance
Pending
$
0.00
Amount
Due
$
89.0!
Current
Account Balance
3,371.78
Insurance
Claims Pending
$
0.00
Current
Amount
Due
$
3,371.71
1VIAYO
CLINIC
200
First
Street
SW
Rochestei
Minnesota
55905
507-284-2511
Fernando
A.
Rivera,
M.D.
June
15,
2007
Division
of
General
Internal
Medicine
Department
of
Internal
Medicine
Mr.
Donald
R.
Sapp
RE:
Mr.
Donald
R.
Sapp
29321
Dutch
Creek
Road
MC#:
5-308-286
R.R.1,Box64
DOB:
1957-8-26
Rockport,
IL
623
70-3046
Dear
Mr.
Sapp:
I
appreciate
the
recent
opportunity
to
see
you
in
General
Internal
Medicine.
I
am
writing
to
provide
a
summary
of
the
medical
findings
at
Mayo
Clinic.
Our
final
diagnoses
were:
•
Obstructive
sleep
apnea
•
Degenerative
arthritis
left
hip
•
Degenerative
arthritis
facet
joint,
low
back
pain
•
Bilateral
high
tone
sensorineural
hearing
loss
•
Gout
•
Medically
complicated
obesity,
status
post
Roux-en-Y
gastric
bypass
•
Vitamin
D
deficiency
•
Iron
deficiency
•
Vitamin
B12
treatment
•
Intertrigo
•
Health
maintenance/preventive
medicine
Attached
is
the
clinical
documentation
which
summarizes
our
impressions
and
recommendations
(Rivera,
Fernando
Alonso:
Jun-2-2007,
Apr-25-2007;
Poirier,
Maria
Kopp:
May-i
1-2007;
Auger,
R
Robert:
May-i
1-2007;
Eggert,
Can
Anne:
May-1-2007;
Hiliman,
Alicia
Allison:
Apr-30-2007;
Oxentenko,
Shawn
Cordell:
Apr-30-2007;
Poppen,
Carroll
F:
Apr-30-2007;
Aitchuler,
Steven
I:
Apr-26-2007).
I
have
also
included
the
most
recent
laboratory
results
report.
GmAT
LAKES
DREDGE
&
DOCK
CoMPANY
Employee
Injury
or
Illness
Questionnaire
1.
Name:
4
‘
M’
2.
Occupation:
.j
E
4ci
c
‘
.5
3.
SS#:
3
?
-
4.
DateofBirth:
—5
2
‘1
..-
.,
..
5
Home
Address
/
5
/
J
fr’
/
/7/1
]‘
..-)
‘7
..
-
&Jr
T
(
.-
.
)
c.
6.
Mailing
Address:
(if
different
from
home
address)
7.
HomePhone#:
l?(3)
.,
7
8.
CellularPhone#:2f
2qa
-
7772
9.
Pager#:
10.
Date
and
time
of
Injury
or
Illness:
/
‘
c
7
/3c
Z’
Ii.
Where
were
you
at
time
of
injury
or
illness?
D,-
c;;
LiL
ç.
12.
Body
Part(s)
injured:
Le
F
‘r
A’-
1
,//—
c
7
13.
What
were
you
doing
when
you
were
injured?
Provide
a
detailed
description
of
how
you
wereinjured:
Lti
f#,,-.U
).-tjj
1i.
1/)
/
3
./p(.
Øi)
JA
-r
/
r
‘_
it,’l/
-‘J
/2
i4k’
A-L).
f
6/f’_
4v
i
fJia-.i.
/-‘t
1’,)
Z’
J4-&.2
-.
/W..
F
t4’
4
•1.T4”/)
jft
1frj
rr
4
14.
Did
you
seek
Medical
Attention:
No
15.
Did
anyone
witness
your
accident?
If
yes)
write
witness
names
below:
&A
r,g
--
-.
)r)/1
4W
-.
Your
Signairi
Today’s
date:
“4
A
1rtfl’,
Revision
0
05811.71)
0flU1/0D0
50001)
flfl72508
DONALD
SAPP
29321
DUTCH
CR RD
ROCKPORT,
IL
62370
I,IIIIs,IIII,II,IIIIIIIII’IIIIIl
Check us
out
online
at
www. orthocenter.
net
You
may
also
email
us
with
your
billing
and
account
concerns
at
billing@orthocenter.net
Please Include Security
Code From Back
Of
Card
cARtI
NUMBER
EXP.
DATE
ARDHOL0ER
NAME
SECURITY
CODE
SIGNATURE
AMOUNT
f
Office Phone
Number
(217)
862—0624
PLEASE
RETURN
THIS PORTION
WITH
PAYME
Statement
Date
Your
/ocount
berPNo.
Patient
Balance
Si-iOW AMOUNT
CHARGES
APPEARING
ON
THIS
STEMENT ARE
NIYE 1NCLUDED ON ANY
HOSPITAL BILL
OR STATEMENT
:AYMN
JJ.CREDUrS
ROMANELLI
MD/MELESKI
DC
CPT:
99244
POS:
11 OFFICE
CONSULT-COM D
SAPP
WOPEEP..S COMP
#
720903
Filed
OVER
60
DAYS CALL
EMPLOYER
c#
7209031
Visit
Totals:
ROMANELLI
MD/ROMANELLI
MD
CPT:
99213
POS:
1]. EST PATIENT-EXPAND
0
SAPP
WORKERS COMP
#
721039
Filed
OVER
60
DAYS CALL
EMPLOYER
c#
ROMA:NELLI
MD/ROMANELLI
MD
CPT: 99213
POS: 11
EST
WORKERS
COMP
#
723271
OVER
60 DAYS CALL
EMPLOYER
c#
7210391
Visit
Totals:
ROMANELLI
MD/ROMA]SIELLI
MD
CPT:
99213
POS: 11 EST
PATIENT-EXPAND 0
SAPP
WORKERS
COMP
#
726501
Filed
ROMANELLI
MD/ROMANELLI
MD
11608 CPT:
99213
P05: 11 EST
PATIENT-EXPAND
0
SAPP
11708 WORKERS
COMP
#
731303
Filed
Billing
inquiries
call
To
schedule
an appointment
(217)
862—0674
(217)
862—0624
0.00
0.00
0.00
0.00
90.00
90.00
Eatement
01/17/08
PLEAE
INDICATE
YOUR ACCOUNT NUMBER
WHEN CALLiNG OUR
OFFICE
00033055
ate:
PATIENT
GALA
PAY THIS
AMC
CONTINUED
END
INQUiRIES
I
PAYMENTS TO:
ORTHOPAEDIC
CENTER
OF ILLINOIS
P0
BOX
2951
SPRINGFIELD
IL
62708
IRS
#:
364156469
(217)
862—0624
THIS
IS NOT A BILL.
IF
THE
BALANCE DUE IS OVER
60 DAYS
OLD,
PLEASE
CONTACT YOUR
EMPLOYER ABOUT
PAYMENT.
081170
00033055
cR1H?FJJIC
cNIER
cE
ILLThVIS
V
B2C
51
!ZrlEW
IL
62708
6231
B5372M
FR1B
BNS
006
1098
P.
CHECK CARD USING
FOP PAYMENT
lj
MASTERCARD
VISh
RMI
tO:
ORTHOPAEDIC
CENTER
OF ILLINOIS
P.O.
BOX
2951
SPRINGFIELD,
IL
62708—2951
I
,II,ijI,IIi,iIIIi.IiiIiiiIiIIIii,I,Iii,,NiIIii,,IIiIi,II
01007
-.1 •fl7
11708
01907
02207
11708
10207
10507
11708
0. 00
0
. 00
0.00
0.00
294
0.00
0.00
0.00
0.00
9C
PATIENT-EXPAND
0
SAPP
Filed
7232711
Visit
Totals:
294.00
294.
00
90.00
90
.00
90.
00
90.00
90.00
90.
00
95.00
12107
12607
Visit Totals:
0.00
95.00
Check
us
out online
at
www.orthocenter.net
You
may also
email
us
with your
billing
and account
concerns
at
6231
billing@
orthocenter
. net
E5
37214
FRi 8
BITS 006
1098 L
PieDse
Include
Security Code
From
Back
Of
Card
CHECK
CARD USiNG
FOR PAYMENT
O
ti
MATERC4RD
.9SA
CARD
NUMBER
EXP.
DATE
CARDHOLDER
NAME
SECURITY
CODE
SIGNATURE
AMOUNT
PLEASE
RETURN
THIS PORTION
WITH
PAYM
Your
Account
Number
‘PaoeNo.
‘T
Patient
Balance
AMOUNT
(217)2-O624LO1/17/O8[
OOO33O55j02474.OOPPJDHERE$
CHARGES
APPEAFUNG
ON THIS
STATEMENT
ARE NOT
INCLUDED
ON ANY
HOSPflAL
BILL
OR STATEMENT
AP C13PJT$
Visit
Totals:
95.00
95.00
0.00
Billing
inquiries
call
To
schedule
an
appointment
(217)
862—0674
(217)
862—0624
EN0 INQUIRIES
/
PAYMENTS
TO:
ORTHOPAEDIC
CENTER
OF
ILLINOIS
P0
BOX
2951
SPRINGFIELD
IL
62708
IRS #:
364156469
(217)
862—0624
THIS
IS NOT
A
BILL.
IF
THE
BALCE
DUE
IS
OVER
60
DAYS
OLD,
PLEASE
CONTACT
YOUR
EMPLOYER
B0UT PAYMENT.
00033055
cRTl-IP?EJIC
cNIER
cF
ILLI2L8
.R) B 51
NEED
IL
62708
OD117O
uanTiUOti
05000
a.aO
DONALD
SAPP
REMIT TO:
ORTHOPAEDIC
CENTER
OF
ILLINOIS
P.O.
BOX
2951
SPRINGFIELD,
IL
62708—2951
liii,.,
111111111111.111.
II I
1111.1 111111111,111
IIIIIIIIIIII
,aiernent
01/17/08
PLEASE
iNDiCATE
YOUR
ACCOUNT
NUIvIBER WHF_N
CALLING OUR
OFFICE:
00033055
)atC.
CURRENT
30-60
DAYS
60-90
DAYS
>
90
DAYS
TOTAL
INS
PENDING
95.00
90.00
180.00
294.00
659.00
185.00
PATIENT
BAL
PAY
THIS
AM
4.;
ORTHOPAEDIC
CENTER
OF
ILLINOIS,
LTD.
RONALD
R.
ROMANELLI,
M.D.
3136
OLD
JACKSONVILLE
ROAD
SPRINGFIELD,
IL
62704
(217)
862-24
NAME
4
1
AGE
ADDRESS
DATE
ii
‘
L/
j;L,.
1
.
3
,4
<*/
U
MAY
SUBSTITUTE
U
DiSPENSe
AS
WRITrEN
Refill
times
_
‘__‘___<_-c-
-_z---(----”
ILLINOIS
ENVIRONMENTAL
PROTECTION
AGENCY
MEMORANDUM
DATE:
February
9,
2005
TO:
DLPC
/
Division
File
FROM:
Paul
Eisenbrandt,
DLPC/FOS
Springfield
Region
SUBJECT:
LPC
#1498005003
—
Pike
County
Rockport/Sapp
C
-05-060-C
FOS File
INSPECTION
DATE:
January
27,
2005
The purpose
of
this
memorandum
is
to
serve
as
the
Narrative
Inspection
Report
Document
of
a
January
27, 2005
complaint
investigation
of
the
above
referenced
site.
The January
18,
2005
anonymous
complaint
alleged
the
owner
had
unlicensed
vehicles
without
titles,
oil
and
diesel
spills,
empty
oil
jugs,
batteries,
and used
tires
littering
the
property.
The
owner
was
also
allegedly burning
household
garbage
and
pushing
the
waste
into
a
tributary
of
the
Big
Dutch
Creek.
The
inspection
took
place
from about
9:58
am
to
11:35
am,
and twenty
digital
photographs
were
taken.
The
weather
was
overcast
with
light
snow
flurries
and approximately
20°F.
Trooper
Thomas
Mavity
(217-285-2034)
and
Trooper
Rich
Avoletta
(217-285-2034),
Illinois
State
Police,
District
20;
Chief
Deputy
Steve
Lehr
(217-285-5011),
Pike
County
Sheriffs
Department;
and
Jane
Johnson
(217-285-4407),
Pike
County
Health
Department,
accompanied
this author
on
the
site
inspection.
Donald
Sapp
(owner)
and
Cheryl
Stewart
(Mr. Sapp’s
sister)
were interviewed
at
the
site
at
the
time
of
the
inspection.
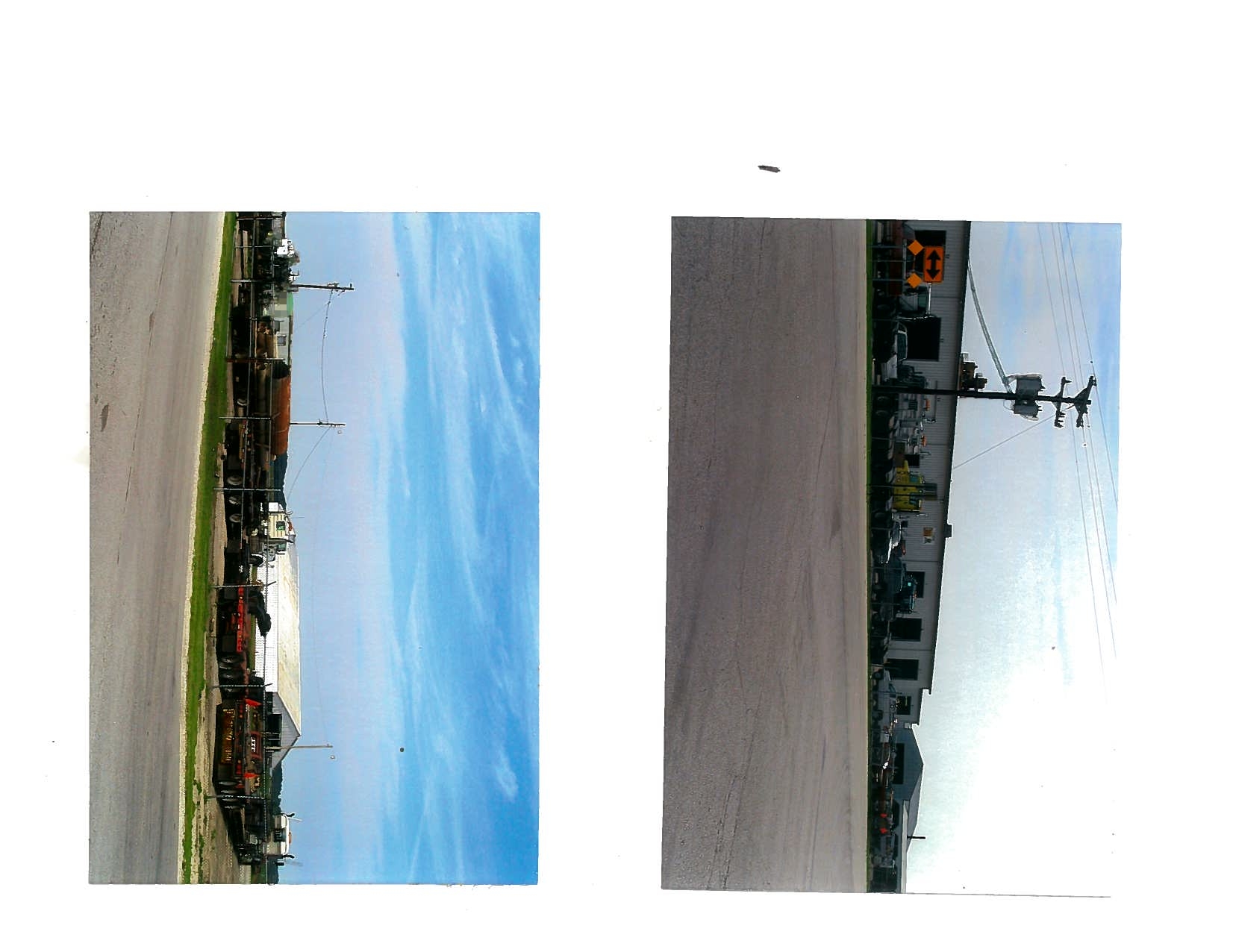
This
approximate
5-acre
site
is
located
at
29321
Dutch
Creek
Road
in
Rockport,
Illinois
(see
attached aerial
photographs).
The
entrance
to
the
driveway
is
on
the
south
side
of
the
road
and
just
west
of
the
Dutch
Creek
Bridge.
The
warranty
deed
lists
the
owner
as
Donald
Sapp.
Donald
Sapp
(217-437-5861,
217-242-7772)
lives
on
the
property.
The
warranty
deed
for
this
property
is
attached
to
this
report.
Photograph
1
shows
a
burn
pile
with
charred
remains
of
aluminum
cans,
tin
cans,
glass
bottles,
plastic
soda
bottles,
Styrofoam
cups,
and
fast
food
wrappers
as
well
as
other
household
waste.
There
were
partially
burnt
blue
jeans,
magazines,
dimensional
lumber,
an
exterior
wood
door,
the
board
and
strings
of
a
piano,
and
a
kitchen
sink.
The
red
and
white
55-gallon
drum
seen
in
the
photograph
was
full
of
new
oil.
Brick
and
miscellaneous
wastes
littered
the area
around
the
burn
pile.
Mr.
Sapp
stated
he
did
not
know
that
burning
waste
was
unlawful.
The
Illinois
EPA
inspector
explained
that burning
domicile
waste
(paper,
cardboard,
etc.)
in
containers
was
permitted
and
that
a
pamphlet
on
burn-barrels
would
be
sent
to
him.
He
was
instructed
not
to
burn
plastic,
food
wrappers,
processed
wood,
etc.
page
1
N
3
*
4
F
7
/